
Mental Health & Stigma
Is Taking GLP-1 Cheating? The Science vs. The Stigma
Edited by Ryan Lafayette. This guide reports public details only and is not medical advice.
Is taking GLP-1 cheating?
No. Obesity is a chronic disease recognized by the AMA. GLP-1 agonists treat a biological dysfunction in the hypothalamus (incretin deficiency), restoring normal satiety signals—not replacing willpower.
✓ Editorial Review
Verified by The Editor
Coach Claire Says
“I know that look.”
It’s the one your aunt gives you across the Thanksgiving table when you pass on the pie. The one that says, “Oh, you’re doing THAT. The easy way.”
And honestly? Sometimes you believe it. Because for the first time, the food isn’t screaming at you. It’s quiet. But when you’ve spent decades fighting a war against your own hunger, peace can feel suspiciously like cheating. You ask yourself: “Is taking GLP-1 cheating?” Let’s talk about why it isn’t.

The “Moral Failure” Myth: Is Taking GLP-1 Cheating?
Here is the dirty little secret regarding GLP-1 medications like Ozempic, Wegovy, and Zepbound: It feels like cheating because, for the first time, the playing field is level.
If you have spent your entire life believing that thin people just have “better character” or “more discipline” than you, taking a medication that suddenly makes you indifferent to a box of donuts feels like you bought a superpower. You didn’t do the “work” of suffering.
But ask yourself this: Does a person with 20/20 vision feel like they are “cheating” because they don’t have to squint? No. Their eyes just work. For those of us with obesity, our metabolic “eyes” don’t focus correctly. GLP-1s don’t play the game for you; they just change the difficulty setting back to Normal.
The Medical Truth: You Can’t “Will” a Hormone
To scientifically answer the question “is taking GLP-1 cheating?”, we must look at the pathophysiology of the disease. In 2013, the American Medical Association (AMA) officially classified obesity as a chronic disease state.1
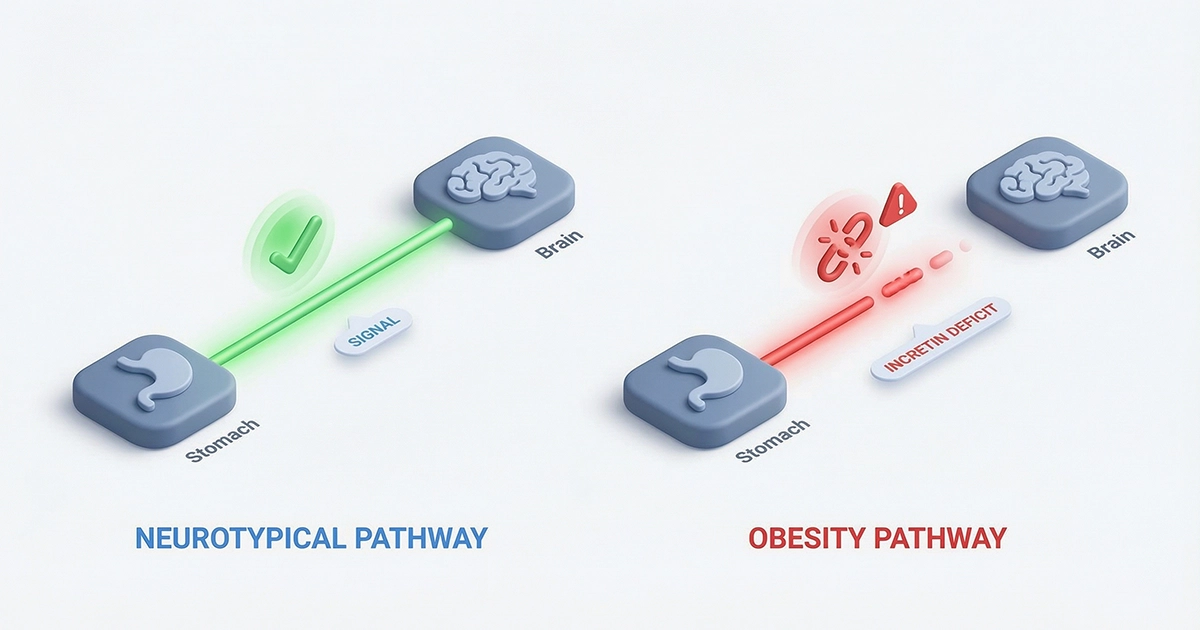
The Incretin Deficit
The core mechanism involves incretins—hormones that signal the brain that you are full. In a neurotypical metabolism, eating triggers a release of GLP-1. This signal tells the brain: Stop eating.2
Clinical data suggests patients with obesity often suffer from a blunted incretin effect. You eat, but your brain never gets the memo. You are not “greedy”; you are chemically deaf to your own satiety.
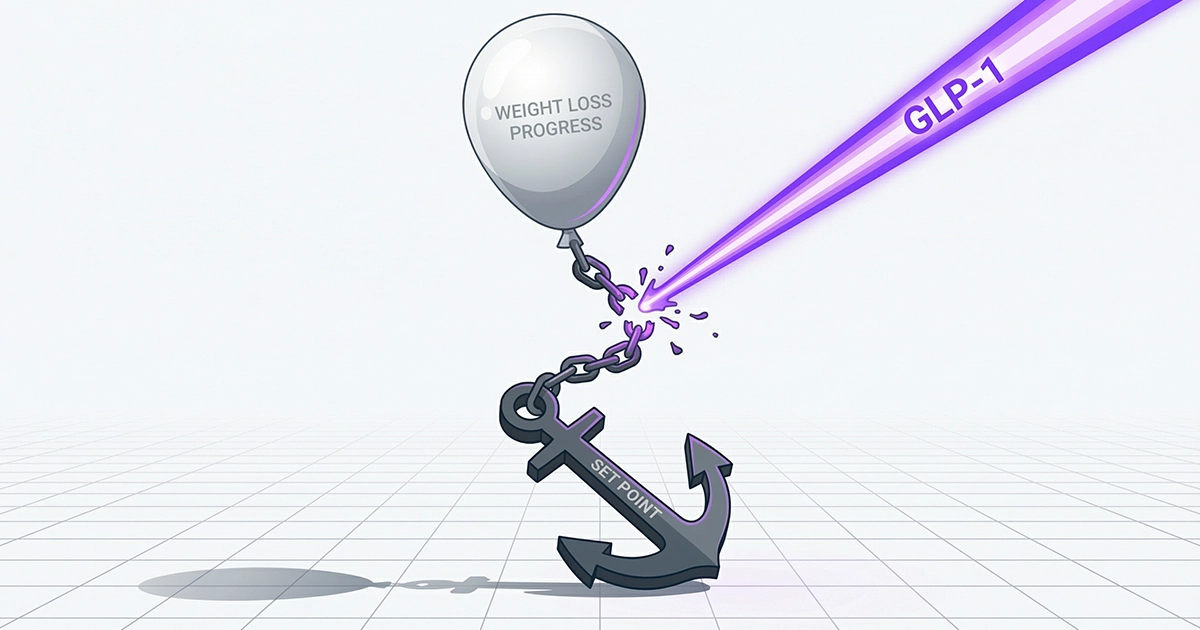
The Set Point Theory
The second hurdle is the Set Point. The hypothalamus acts like a thermostat. If you lose weight through diet alone, your body perceives this as starvation and fights back by increasing hunger hormones (ghrelin).3
| Metric | Diet & Exercise Alone (Willpower) | GLP-1 Therapy (Biology) |
|---|---|---|
| Mechanism | Caloric deficit via conscious restriction. | Restored satiety signaling. |
| Response | Body slows metabolism (Defense). | Body accepts lower weight (Reset). |
| Food Noise | Increases. | Silenced. |
The “Easy Way Out” Fallacy: Debunking the Critics
Critics often argue that medication is a “shortcut.” This ignores the clinical reality of chronic disease management.
Myth: “You can just stop once you reach your goal.”
The Medical Fact: Obesity is a chronic, relapsing disease. The STEP 1 Extension Study demonstrated that participants who stopped semaglutide regained two-thirds of their lost weight within one year.4
The Reality: The medication is not a cure; it is a treatment. Just as blood pressure returns when you stop meds, appetite dysregulation returns when GLP-1s are withdrawn.
The Social Survival Guide
Let’s get back to the dinner table. Your Aunt Linda doesn’t care about the hypothalamus. She cares about judgment.

When people accuse you of cheating, your instinct is to defend yourself. Don’t. You do not owe anyone a PowerPoint presentation on your medical history.

Use the Cut & Comeback Protocol. Keep it calm, confident, and brief. Think James Bond, not Debate Team.
Cuts & Comebacks
The Cut: “Must be nice to just take a shot and lose weight.”
The Comeback: “It is nice. I’m finally treating a medical issue. Pass the turkey?”
The Cut: “You’re taking that medicine away from diabetics.”
The Comeback: “Actually, I use a dedicated supply chain. No shortage impact. I checked.”
The Cut: “Why don’t you just eat less? It’s simple math.”
The Comeback: “The math works, but my biology didn’t. Now it does.”
The Cut: “Be careful. That stuff is basically anorexia in a pen.”
The Comeback: “It’s actually satiety, not starvation. I feel full, not fearful.”
The Cut: “You’ll have to be on drugs forever.”
The Comeback: “Maybe. Chronic issues require chronic care. I’m good with it.”
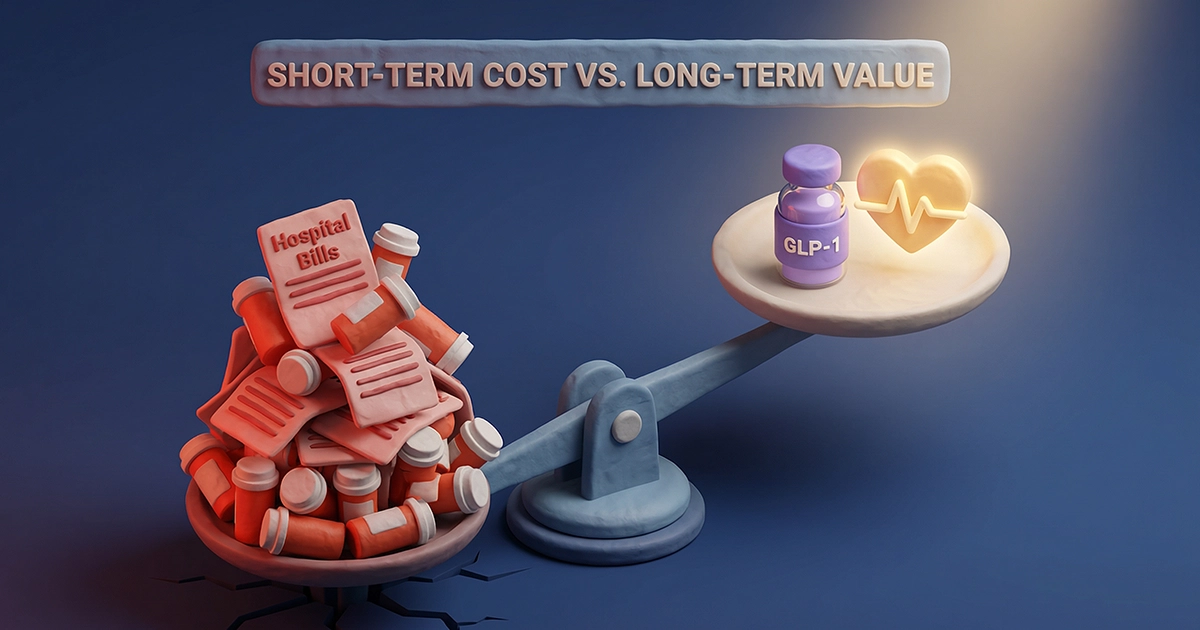
Is It Worth the Cost?
Finally, “cheating” implies getting something for nothing. But GLP-1 therapy is an investment.
Compounded Semaglutide (Starter Tier)
Editor Verified
Cash Pay
$297/mo
Month 1 (Median)
Consultation
Included
Medication
Included
Compare Providers
*Composite median based on Hims, Mochi, and Orderly offers. Prices vary by state.
The Bottom Line: You Aren’t Cheating, You’re Healing
When you treat a broken bone, nobody asks if you “earned” the cast. They understand that the cast supports the healing process so the body can do its job. GLP-1s are the cast for your metabolism. The diet and exercise? That’s the physical therapy. You need both.
So the next time that voice of doubt creeps in—whether it’s from your own head or Aunt Linda’s dinner table conversation—remember this: If you ask “is taking GLP-1 cheating?“, the answer is a hard no. You aren’t cutting corners. You are correcting a biological deficit so your hard work finally counts. That’s not cheating. That’s healthcare.
Medical Disclaimer: This content is for educational purposes only and has been verified against clinical data for accuracy. It does not constitute medical advice, diagnosis, or treatment. Always consult your prescriber or healthcare provider before starting or changing any GLP-1 medication regimen.
References
- American Medical Association. Resolution 420 (A-13): Recognition of Obesity as a Disease. 2013.
- Holst JJ. The physiology of glucagon-like peptide 1. Physiological Reviews. 2007;87(4):1409-1439.
- Sumithran P, et al. Long-term persistence of hormonal adaptations to weight loss. N Engl J Med. 2011;365(17):1597-1604.
- Wilding JPH, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes Obes Metab. 2022;24(8):1553-1564.
- Garvey WT, et al. American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Clinical Practice Guidelines for Medical Care of Patients with Obesity. Endocr Pract. 2016;22(Suppl 3):1-203.
- Jastreboff AM, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387(3):205-216.
- U.S. Food and Drug Administration. FDA Approves New Drug Treatment for Chronic Weight Management, First Since 2014. FDA Press Release. 2021.
- Volkow ND, et al. Obesity and addiction: neurobiological overlaps. Obes Rev. 2013;14(1):2-18.
- Müller TD, et al. The physiology of incretins: from the enteroendocrine cell to the clinic. Nat Rev Endocrinol. 2019;15:606-626.
- National Institute of Diabetes and Digestive and Kidney Diseases. Health Risks of Overweight & Obesity. NIH Publication. 2023.