Ozempic Stopped Working? Plateau Questions to Discuss With Your Clinician
THE BOTTOM LINE
If you feel like Ozempic stopped working, you are likely experiencing a plateau caused by biological tolerance (tachyphylaxis) or injection site issues, not a lack of willpower.
- The Cause: Receptors may downregulate after 6+ months, or scar tissue may be blocking absorption.
- What to ask: Rotate injection sites to optimize protein timing for "Day 5 Hunger," or consult your provider about switching to a dual-agonist like Mounjaro.
- The Warning: Do not split doses without medical supervision; this increases infection risk and treatment planning errors.
What This Plateau Review Covers
- How To Tell Whether Weight Loss Has Truly Stalled
- Which Common Plateau Causes Are Behavioral Versus Pharmacologic
- When A Dose, Routine, Or Nutrition Review May Help
- When To Escalate The Discussion With Your Prescriber
Why This Happens: The Biology Behind the Stall
When patients report that Ozempic stopped working, they are often describing a physiological phenomenon known as tachyphylaxis. In simple terms, this is a rapidly diminishing response to successive doses of a drug, rendering it less effective over time 1.
Think of GLP-1 medications like spending an extended time in a completely different climate. At first, you're freezing cold or extremely hot. After a while, the body 'acclimates' to this change even though the climate remains constant.
Receptor Downregulation
The mechanism behind this is receptor downregulation. Your body is becoming accustomed to the medication, and as a result the following may occur:

To break this cycle, we cannot simply "try harder." We must introduce a pattern interrupt-either by changing where we inject, what we inject, or how we support the metabolic baseline.
Start Quiz
Find your best GLP-1 match
If your current plan stalled, what should compare check first?
Checking next-step support?
Compare follow-up options
Coach Claire says:
For the first few months, it felt like magic, didn't it? The "food noise" vanished, and the scale finally moved. But now, despite doing everything right, the numbers are stuck. Take a deep breath and do NOT panic.
Your body is just smart. It's adapting to the medication, a phenomenon we call the "Ozempic Plateau." The good news? We can outsmart the adaptation, by understanding how to optimize the mechanics and biology behind the stall and get that scale moving again.
Address #1: The "Lump Check" Care plan discussion (Lipohypertrophy)
Before adjusting your dose, you must first review your injection technique. A common, yet frequently overlooked cause of medication failure is injecting into scar tissue.
If you have injected into the same site every week for a year, you have likely developed micro-scarring. Repeated injection of medication in the same spot can lead to lipohypertrophy. Injecting into this rubbery tissue can reduce medication absorption significantly, meaning you aren't actually getting your full dose 2.
The "Press and Palpate" Test
To determine if this might be why Ozempic stopped working, perform this self-exam:
- Lie flat on your back.
- Press firmly on your usual injection sites.
- Feel for a "rubbery" texture or a lump that feels denser than the surrounding fat. It is usually not painful.
- The Rule: If you feel a lump, that site is "burned" for at least 3-4 weeks. Stop injecting in that area and read on to refresh on the correct injection method.
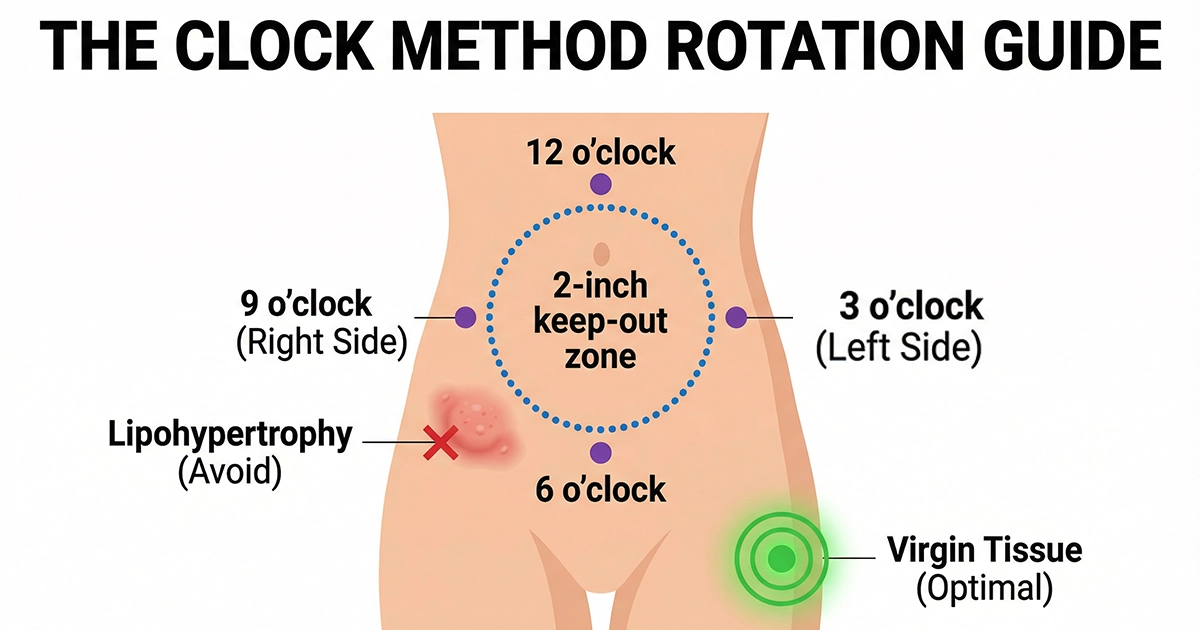
The "Clock Method" Solution
To ensure consistent absorption, adopt the Clock Method for site rotation:
- Week 1: 12 o'clock (Above navel)
- Week 2: 3 o'clock (Left side)
- Week 3: 6 o'clock (Below navel)
- Week 4: 9 o'clock (Right side)
While clinical data suggests semaglutide has similar bioavailability across the abdomen, thigh, and arm, anecdotal evidence suggests that moving to "virgin" tissue (like the thigh) can break a stall simply by avoiding sub-clinical scar tissue in the stomach 3. And always make sure you stay at least 2" from your navel.
Address #2: The Metabolic Audit (Cortisol & Calories)
If your biology is functioning and your injection site is clean, the stall may be metabolic. Paradoxically, the issue is often that patients are eating too little, not too much.
The Starvation Mode Paradox
When caloric intake drops drastically (e.g., below 1,000 calories/day) for extended periods, the body perceives a famine. This triggers evolutionary defense mechanisms:
| Starvation Response | Mechanism |
|---|---|
| To conserve energy, your body reduces its resting metabolic rate-the calories burned just to keep you alive. It becomes more "efficient" at storing fat and burning fewer calories for everyday tasks. | |
| Drastic calorie deficits often cause the body to break down muscle for energy instead of fat. Since muscle is metabolically active, losing it further lowers your daily calorie burn. | |
| Your body may upregulate ghrelin (the hunger hormone) and downregulate leptin (the fullness hormone) to drive you toward eating more, even while you are still taking the medication. | |
| With extremely low energy intake, you may unconsciously move less throughout the day (fidgeting less, sitting more), further decreasing total energy expenditure. |
A landmark study on "The Biggest Loser" participants confirmed that extreme caloric restriction can depress metabolic rate for years, even after weight stabilizes 4. If you have been "white-knuckling" through hunger, your weight loss may have stalled because your body has clamped down on energy expenditure.
What to ask: "Day 5" Protein Loading
Instead of restricting calories, focus on Protein Pacing. GLP-1 medications have a half-life of approximately 1 week (~165 hours), meaning levels drop naturally on Days 5, 6, and 7 5.
- Strategy: On days 5 and 6, increase protein intake to 30g per meal. This physically distends the stomach and triggers satiety hormones (PYY) that the waning medication can no longer stimulate as strongly.
Address #3: The "Hydration-Lipolysis" Link
One of the most ignored factors when Ozempic stopped working is hydration status. The chemical process of burning fat, known as lipolysis, is hydrolysis-dependent. This means water molecules are required to interact with triglycerides to break them down into glycerol and fatty acids.
The "Dry Stall"
The hypothalamus regulates our hunger and thirst centers, so when you're using GLP-1 medications, that loss of food craving can also cause a loss of the need to hydrate and result in chronic dehydration.
- The Science: Without adequate water, the kidneys cannot filter toxins efficiently, forcing the liver to take over some of that load. Since the liver is responsible for metabolizing stored fat, diverting it to filtration duties slows down weight loss 6.
- The Ask your clinician about: Aim for half your body weight in ounces of water daily. If you weigh 200 lbs, your baseline is 100 oz.
Address #4: The "Mounjaro Switch" (Dual-Agonist Therapy)
If you have maximized your semaglutide dose (2.0 mg Ozempic or 2.4 mg Wegovy) and the scale hasn't moved for 8 weeks, clinical consensus suggests switching molecules.
Why Switch to Tirzepatide?
Ozempic is a mono-agonist. Mounjaro (tirzepatide) is a dual-agonist, targeting both GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptors.
This "synergistic" effect recruits a second pathway to regulate energy balance and fat metabolism.
- The Data: In the SURPASS-2 clinical trial, patients on the highest dose of tirzepatide (15 mg) lost an average of 12.4 kg (27.3 lbs), compared to 6.2 kg (13.7 lbs) on semaglutide (1 mg) 7.
- The Logic: If your GLP-1 receptors are downregulated, attacking the weight via the GIP pathway offers a "backdoor" to restart fat loss.

Safety Warning: The "Split Treatment Planning" Myth
When Ozempic stopped working for some patients, online forums popularized the idea of "splitting the dose" (e.g., taking half the dose on Monday and half on Thursday) to manage hunger.
Medical Reality: This practice is NOT FDA-reviewed and carries significant risks.
- Infection Risk: Standard pens are designed for single-use needles. Re-entering the pen's needle repeatedly or manipulating the mechanism increases the risk of bacterial contamination 8.
- Treatment Planning Inaccuracy: Ozempic pens rely on a "click" mechanism that is not calibrated for partial doses. "Counting clicks" can lead to incorrect treatment planning, causing either ineffective treatment or severe hypoglycemia.
The Pivot: If you're feeling like Ozempic just isn't working for you anymore, discuss switching to a weekly medication with a longer effective duration or higher potency (like Mounjaro) with your doctor rather than playing weight loss roulette and manipulating the injection hardware.
Cost Comparison: Official List Price Context
Breaking a plateau often requires a financial decision. These official list prices give a clean branded baseline before insurance, coupons, or rebates.
| Feature | Ozempic (Semaglutide) | Mounjaro (Tirzepatide) |
|---|---|---|
| Mechanism | Mono-Agonist (GLP-1) | Dual-Agonist (GLP-1 + GIP) |
| Efficacy (High Dose) | ~15% Body Weight Loss 7 | ~21% Body Weight Loss 7 |
| Official List Price | $997.58 / 28-day supply | $1,112.16 / 28-day supply |
| Right For | Maintenance / T2DM Control | Breaking Plateaus / High BMI |
COACH CLAIRE SIGN-OFF
Hitting a plateau is frustrating, but it's also a sign that your body has adjusted to its new normal. That's actually a biological victory! Whether you choose to rotate your injection site, prioritize protein on "hungry days," or talk to your doctor about the Mounjaro switch, remember: A stall is not a stop. It's just a signal to change gears. Don't panic! You've got this.
Coach Claire's Cheat Sheet
Quick definitions used in this article.
Frequently Asked Questions
Does rotating injection sites really help weight loss?
Yes. Injecting into "virgin" tissue avoids scar tissue (lipohypertrophy) that blocks absorption. While semaglutide itself is effective across injection sites, avoiding scarred areas ensures you receive the full intended dose 23.
Is it safe to split my Ozempic dose?
No. Splitting doses involves using uncalibrated "click" methods and often requires reusing needles or manipulating the pen, which significantly increases the risk of treatment planning errors and bacterial infections 8.
Can I switch from Ozempic to Mounjaro immediately?
Yes, but usually at a lower starting dose. Because Mounjaro introduces a second hormone (GIP), providers typically start patients at 2.5 mg or 5 mg to mitigate gastrointestinal side effects, even if they were on a high dose of semaglutide.
Why do I get hungry on Day 5?
Semaglutide has a half-life of approximately 7 days. By days 5, 6, and 7, the concentration of the drug in your blood naturally decreases, allowing appetite signals to return before your next scheduled dose 5.
References
- Lehne, R. A. (2013). Pharmacology for Nursing Care. Saunders. (Definition of Tachyphylaxis). [top]
- American Diabetes Association (ADA). (2024). Insulin and GLP-1 Injection Technique Guidelines. Diabetes Care. [top]
- Food and Drug Administration (FDA). (2017). Ozempic (semaglutide) Clinical Pharmacology Review. FDA.gov. [top]
- Fothergill, E., et al. (2016). Persistent metabolic adaptation 6 years after "The Biggest Loser" competition. Obesity. [top]
- Food and Drug Administration (FDA). Ozempic (semaglutide) Prescribing Information. [top]
- Thornton, S.N. (2016). Increased Hydration Can Be Associated with Weight Loss. Frontiers in Nutrition. [top]
- Frías, J.P., et al. (2021). Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes. New England Journal of Medicine (SURPASS-2). [top]
- Centers for Disease Control and Prevention (CDC). Injection Safety: FAQs regarding safe needle practices. CDC.gov. [top]