GLP-1 vs. Bariatric Surgery: Cost, Results, and Regain Risk Questions
THE BOTTOM LINE
The decision between GLP-1 vs bariatric surgery is no longer binary. It is a decision between Mechanical Restriction (Surgery), Hormonal Regulation (Medication), or the increasingly common Hybrid Approach.
- Efficacy: Surgery remains the "Gold Standard" for massive weight loss (30-35%), while GLP-1s like Tirzepatide are closing the gap (21%).
- Economics: Surgery is a high one-time investment ($15k+). GLP-1s are a low monthly cost that becomes more expensive than surgery after Year 2.
- Safety: Surgery carries acute operative risks. GLP-1s carry chronic GI risks and a critical anesthesia aspiration risk.
- The Future: Data suggests the most durable long-term outcome for severe obesity may be surgery followed by low-dose medication maintenance.
What This Comparison Review Covers
- How Medication And Surgery Differ In Expected Weight-Loss Magnitude
- What Regain, Durability, And Adherence Tradeoffs Matter Most
- Which Risks, Recovery Demands, And Side Effects Change The Choice
- Which Patient Questions Belong In A Clinician-Led Decision
The Efficacy Gap: Does the Needle Finally Match the Knife?
For thirty years, the gap between "diet and exercise" (typically 3-5% weight loss) and "bariatric surgery" (25-30% weight loss) was a canyon that no pill could cross. Modern GLP-1 Receptor Agonists have finally built a bridge across that canyon, but looking at the raw data, they haven't closed the gap entirely.
The Head-to-Head Clinical Data
To understand GLP-1 vs bariatric surgery efficacy, we must look at the gold-standard trials. According to a 2024 comparative analysis by the American Society for Metabolic and Bariatric Surgery (ASMBS) and data from the SURMOUNT-1 trial, the hierarchy is distinct13:
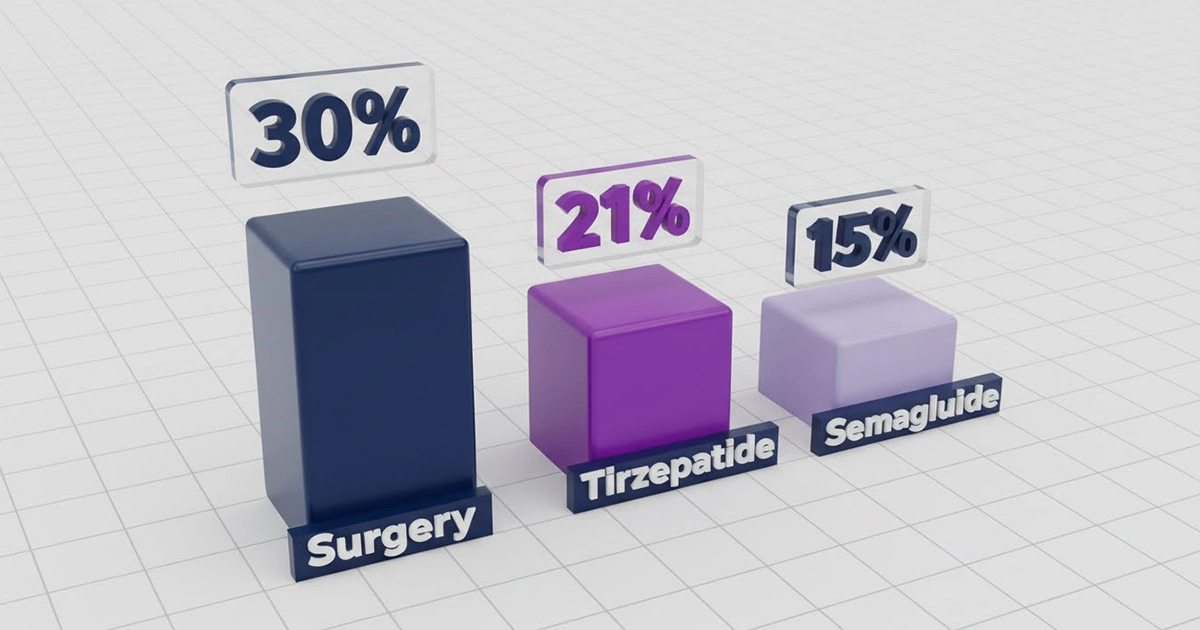
- Gastric Bypass (Roux-en-Y): The metabolic heavyweight. It yields ~30-35% Total Body Weight Loss (TBWL). It combines restriction (smaller stomach) with Malabsorption.
- Gastric Sleeve (VSG): The most common procedure globally, yielding ~25% TBWL. It is purely restrictive but creates a hormonal shift by removing the stomach fundus (the hunger center).
- Tirzepatide (Zepbound?): The first dual GIP/GLP-1 agonist. In the SURMOUNT-1 trial, the 15mg dose achieved 20.9% TBWL over 72 weeks3. This is the closest medication has ever come to surgical results.
- Semaglutide (Wegovy?): The standard GLP-1 agonist. The STEP-1 trial demonstrated 14.9% TBWL over 68 weeks2. Effective, but statistically inferior to both surgery and Tirzepatide for massive weight loss.
The "Real World" Adherence Drop
It is critical to distinguish between efficacy (what happens in a controlled trial) and effectiveness (what happens in your chaotic life).
In surgery, compliance is engineered into your anatomy. You cannot "forget" to have a small stomach. The restriction is physical and permanent. With GLP-1s, effectiveness relies on filling prescriptions, managing nausea, finding stock during shortages, and affording the copay. Consequently, real-world data often shows medication weight loss hovering closer to 5-10% long-term due to discontinuation rates4.
Start Quiz
Find your best GLP-1 match
What should compare prioritize first?
Comparing medications next?
Compare GLP-1 providers
Coach Claire says:
It is the #1 question of 2026: "Why go under the knife when I can just take a shot?"
For decades, the choice was binary: 1) diet and fail or 2) surgery and stigma. Today, we're still having the "Needle vs. Knife" debate. But what if I told you there's another path? Instead of either/or, these two options can co-exist as teammates.
One alters your anatomy to create a metabolic reset; the other acts as a hormonal shield to protect that result. The real question is: which one solves your specific metabolic breakdown? Let's dig into the safety, costs, and the "Synergy" strategy to help you make well-informed choices on your weight loss journey.
Mechanism of Action: Plumbing vs. Signal
Why does surgery still win on durability? It comes down to the difference between altering the "hardware" (anatomy) versus the "software" (hormones).
Surgery: Cutting the Wire (The Metabolic Reset)
Bariatric surgery is often called a "metabolic reset." By physically removing the fundus of the stomach (in a Sleeve Gastrectomy), the surgeon removes the primary factory for Ghrelin, the "hunger hormone." This isn't just about making the stomach smaller; it is about silencing the chemical scream that tells your brain to eat.
Furthermore, procedures like the Bypass alter the gut microbiome and bile acid flow, increasing natural GLP-1 secretion by over 300% post-prandially5. You are essentially turning your own body into a GLP-1 factory.
Medications: Muting the Volume (The Maintenance Signal)
GLP-1 medications are synthetic mimics. They don't change your anatomy; they flood your receptors with a signal that says, "We are full."
Think of it like a fire alarm. Surgery cuts the wire to the alarm. GLP-1s put a heavy blanket over the speaker to muffle the sound. The moment you stop taking the medication, the blanket is lifted, and the alarm (your natural hunger) begins to ring again (and often louder than before).
The Psychology of Hunger: Brain vs. Belly
A critical factor often overlooked in the GLP-1 vs bariatric surgery decision is where the intervention happens: in the gut or in the brain?
The "Food Noise" Factor
Many patients suffer from "Food Noise": intrusive, obsessive thoughts about food that persist even when physically full.
- GLP-1s (The Brain Specialist): Drugs like Ozempic and Mounjaro cross the blood-brain barrier. They bind to receptors in the hypothalamus (appetite regulation) and the mesolimbic system (reward/addiction). They are exceptionally good at quieting "Food Noise." You simply don't care about the donut.
- Surgery (The Belly Specialist): Surgery creates physical restriction. If you eat too much, you will vomit (dumping syndrome or regurgitation). It forces you to stop eating, but it does not necessarily stop you from wanting to eat.
The Risk of Transfer Addiction123
Because surgery restricts volume but doesn't fully dampen the dopamine reward system in the brain, some surgical patients experience Transfer Addiction. Studies suggest post-bypass patients may be over 2x more likely to develop alcohol use disorders compared to the general population64.
Conversely, GLP-1s are currently being studied for their potential to cure addiction, as they seem to blunt the dopamine spike not just from food, but from alcohol and shopping as well. If your struggle is primarily psychological craving rather than physical capacity, GLP-1s may offer a unique advantage over the "mechanical" solution of surgery.
Safety Alert: The "Anesthesia Trap" (Crucial 2026 Update)
ASA Safety Warning
If you are considering surgery-whether it's bariatric, plastic surgery, or a knee replacement-while taking these drugs, you must understand the ASA Safety Warning.
Many patients attempt to "supercharge" their pre-op weight loss by taking GLP-1s right up to their surgery date. This is dangerous.
The Mechanism: Delayed Gastric Emptying
GLP-1s work by slowing down digestion (gastroparesis). This keeps food in your stomach for hours, or even days, longer than normal. Standard anesthesia care plan discussions require you to fast for 8-12 hours to ensure an empty stomach. However, for a patient on Ozempic or Mounjaro, an 8-hour fast is often insufficient. Food may still be present in the stomach.
The Risk: Pulmonary Aspiration
If there is food in your stomach when you are sedated, you risk Pulmonary Aspiration. This is a life-threatening complication.
The ASA Care plan discussion (Stop Dates)
The American Society of Anesthesiologists (ASA) has issued strict guidance7:
- Daily Meds (e.g., Rybelsus, Saxenda): Hold for 24 hours before surgery.
- Weekly Injectables (e.g., Ozempic, Wegovy, Mounjaro, Zepbound): Hold for one week before surgery.
Always disclose your GLP-1 use to your anesthesiologist. They may perform a gastric ultrasound to ensure safety before putting you under.

The Hidden Maintenance: Vitamins and Malabsorption
While much is made of the "monthly maintenance" of GLP-1 injections, bariatric surgery comes with its own lifelong maintenance ask your clinician about: Nutritional Surveillance.
The Surgical Vitamin Tax
Because bariatric surgery (specifically the Bypass and Duodenal Switch) works by intentionally causing malabsorption, the body loses the ability to absorb certain nutrients efficiently from food.
- The Commitment: You must take bariatric-grade multivitamins, Calcium Citrate (not Carbonate), Iron, and B12 forever.
- The Consequence: Missing these vitamins can lead to neuropathy, movement disorders, and cognitive impairment. Other consequences include severe anemia, osteoporosis, and tooth loss. Taking these vitamins is not optional; it is a medical requirement8.
The GLP-1 Nutritional Reality
GLP-1s do not cause malabsorption. You absorb nutrients normally; you just eat less volume.
- The Advantage: You generally do not need specialized "bariatric" vitamins, though a high-quality multivitamin is recommended to cover gaps caused by low caloric intake.
- The Risk: The primary nutritional risk with GLP-1s is simply under-eating protein and fiber, leading to muscle loss and constipation, rather than the specific micronutrient deficiencies seen in surgery.

The Hybrid Model: Why Not Both?
We often frame this as an "Either/Or" battle, but the future of obesity medicine is Combination Therapy.
The "Neoadjuvant" Care plan discussion (Meds Before Surgery)
Some surgeons are now using GLP-1s before surgery to reduce liver volume and surgical risk in super-obese patients (BMI > 60).
- The Goal: Reduce the BMI to a safer range for anesthesia and laparoscopic access.
- The Caution: As noted in the Safety Alert, these meds must be strictly stopped prior to the actual procedure day to clear the stomach.
- The Verdict: It is not a failure to use medication after surgery. It is utilizing two different tools to treat a chronic, relapsing disease.3
Post-Surgery: The "After" Care plan discussion
Surgical patients who experience weight regain (typically 3-5 years post-op) are now prime candidates for GLP-1s.
- Why it works: The surgery has already debulked the weight and created restriction. The GLP-1 addresses the "metabolic adaptation" (the slowing of metabolism) and the return of hunger hormones.
- The Data: Recent real-world studies indicate that post-bariatric patients who add a GLP-1 can lose an additional 14.8% of their recurrent body weight, effectively reversing the "bounce back"9.
Rent vs. Buy: The Financial Crossover
This is a financial decision between a "Mortgage" and "Rent." The economics depend entirely on your insurance coverage, but let's look at the cash-pay reality for those without coverage.
Surgery: The "Buy" (High Upfront, Low Maintenance)
- Cost: $15,000 - $22,000 (Cash Pay Average in US).
- Recurring Cost: Vitamins ($30/mo).
- ROI: This is a one-time metabolic event. Once the anatomy is altered, you own the "tool" for life.
GLP-1s: The "Rent" (Low Upfront, Infinite Maintenance)
- Cost: ~$1,000 - $1,300 per month (Brand Name, Cash Pay).
- Recurring Cost: $12,000 - $15,000 per year.
- ROI: You are renting the metabolic effect. The moment you stop paying, the biology fights back.
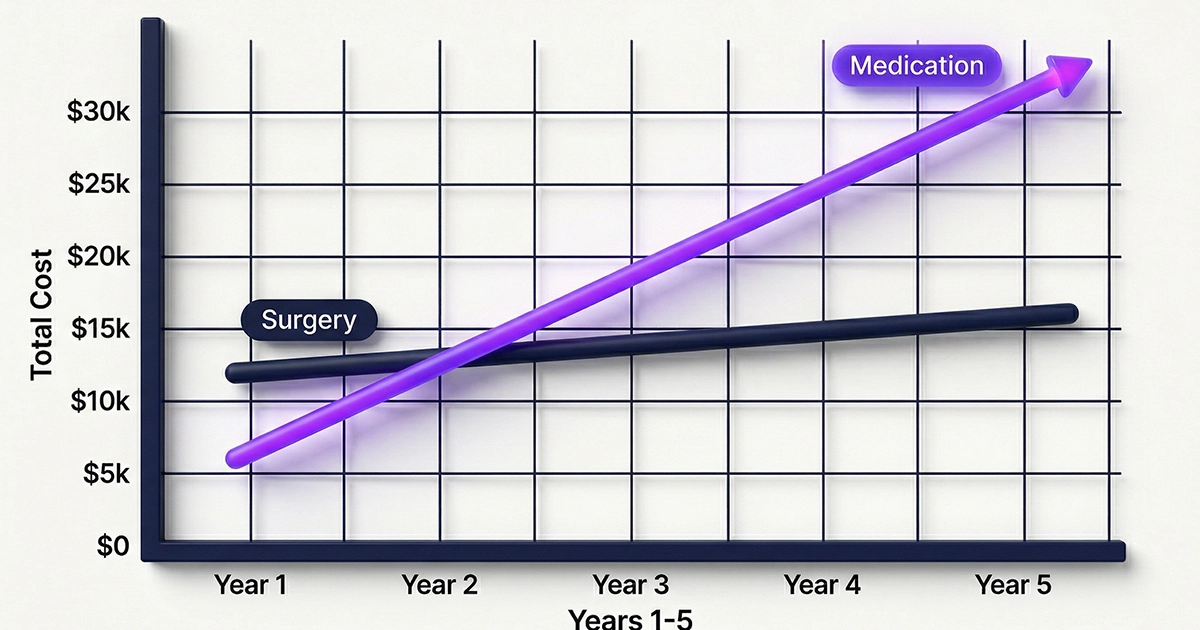
The Break-Even Analysis
If paying cash, the cost of GLP-1s exceeds the cost of bariatric surgery around the 18 to 24-month mark.
- Year 1: Surgery costs $18,000 versus Meds cost $14,000. (Surgery is more expensive).
- Year 3: Surgery costs $19,000 versus Meds cost $42,000. (Meds are double the cost).
- Year 5: Surgery costs $20,000 versus Meds cost $70,000. (The gap widens significantly).
(Note: Surgical costs include estimated vitamin maintenance; Medication costs assume brand-name list price without insurance or savings cards).
Biology Fights Back: The Reality of Regain
The "Bounce Back" is the single most common fear. While both interventions face the challenge of metabolic adaptation, the mechanisms of regain differ.
Medication Regain (Rapid & Acute)
Regain after stopping GLP-1s is typically acute and aggressive. The STEP-1 extension study demonstrated that patients who withdrew from semaglutide regained two-thirds of their lost weight within one year10. Because the medication treats the chronic disease only while it is in your system, "food noise" often returns with greater intensity once the drug clears (typically 5-7 weeks).
Surgical Regain (Gradual & Behavioral)
Regain after surgery is common but typically gradual. Long-term data from the Swedish Obese Subjects (SOS) study shows patients maintaining >50% of their excess weight loss 10-15 years post-op11. However, 20-25% of surgery patients do experience significant regain over time due to behavioral drift and metabolic adaptation (the body learns to outsmart the restriction).
| Metric | Gastric Sleeve (VSG) | GLP-1s (Life-long) |
|---|---|---|
| Mechanism | Anatomical Restriction + Hormonal Reset | Receptor Agonism (Signal Mimicry) |
| Expected Weight Loss | 25% - 30% Total Body Weight | 15% (Semaglutide) - 21% (Tirzepatide) |
| Food Noise | Moderate reduction (Ghrelin reduction) | High reduction (Brain receptor targeting) |
| Reversibility | Permanent (Anatomy Altered) | Fully Reversible (Stop Meds) |
| Cost Model | "One-time Mortgage" ($15k - $20k) | "Monthly Rent" ($12k/year) |
| Anesthesia Risk | Standard Surgical Risk | High Aspiration Risk (Must stop meds) |
| Vitamin Needs | High (Strict lifelong care plan discussion) | Low (Standard multivitamin) |
| Downtime | 2-4 Weeks Recovery | Zero (Nausea potential) |
Coach Claire Sign-Off
Here is the reality, friend. There is no "cheating" here. Whether you choose the tool (surgery) or the fuel adjustment (meds), you still have to drive the car. Surgery forces compliance; meds require you to choose it every single week.
If you are scared of the permanence of surgery, try the meds first. If you are scared of the cost and dependence of meds, talk to a surgeon. Just don't let the fear of "how" keep you from starting.
Coach Claire's Cheat Sheet
Quick definitions used in this article.
Frequently Asked Questions
Can I use GLP-1s if I've already had bariatric surgery?
Yes. This is becoming the standard of care for post-op regain. The mechanisms work synergistically. Many patients find that even low doses of GLP-1s are incredibly effective after surgery because their anatomy already supports restriction.
Is the recovery time different?
Yes. Surgery requires 2-4 weeks off work for physical healing and a strict liquid diet phase. GLP-1s require zero downtime, though nausea and GI distress may impact daily life significantly during the first 4-8 weeks of titration.
Does insurance cover both?
Coverage varies. Many plans cover surgery more readily than chronic weight loss medication due to the defined 'one-time' cost versus a lifetime subscription. However, access to GLP-1 coverage is expanding rapidly for patients with Type 2 Diabetes.
References
- Eisenberg, D., et al. (2022). 2022 American Society for Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO): Indications for Metabolic and Bariatric Surgery. Surgery for Obesity and Related Diseases. [top]
- Wilding, J. P. H., et al. (2021). Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). The New England Journal of Medicine. [top]
- Jastreboff, A. M., et al. (2022). Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). The New England Journal of Medicine. [top]
- Khunti, K., et al. (2023). Real-world adherence and persistence with GLP-1 receptor agonists in patients with type 2 diabetes. Diabetes, Obesity and Metabolism. [top]
- Nielsen, M.S., et al. (2026). Greater early postprandial GLP-1 increase after Roux-en-Y than one-anastomosis gastric bypass. International Journal of Obesity. [top]
- Ostlund, M.P., et al. (2013). Psychiatric diagnoses and suicide attempts before and after gastric bypass surgery. JAMA Surgery. [top]
- American Society of Anesthesiologists. (2023). Consensus-Based Guidance on Preoperative Management of Patients on Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists. [top]
- Mechanick, J.I., et al. (2020). Clinical Practice Guidelines for the Perioperative Nutrition, Metabolic, and Nonsurgical Support of Patients Undergoing Bariatric Procedures - 2019 Update. Obesity (Silver Spring). [top]
- Elmaleh-Sachs, A., et al. (2025). Real-World Effectiveness and Safety of GLP-1 Receptor Agonists in Patients with Weight Recurrence After Bariatric Surgery. JAMA Network Open. [top]
- Wilding, J. P. H., et al. (2022). Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes, Obesity and Metabolism. [top]
- Sj?str?m, L., et al. (2007). Effects of Bariatric Surgery on Mortality in Swedish Obese Subjects. The New England Journal of Medicine. [top]
Medical Disclaimer: This content is for educational purposes only and has been verified against clinical data for accuracy. It does not constitute medical advice, diagnosis, or treatment. Always consult your prescriber or healthcare provider before starting or changing any GLP-1 medication regimen, especially if considering surgery. Medically reviewed by Jane Rivers.