
?
How GLP-1 Medications Work The Science of Appetite, Blood Sugar, and Weight Loss
THE BOTTOM LINE
- What they are: GLP-1 receptor agonists are medications that mimic a natural incretin hormone your gut releases after you eat, called glucagon-like peptide-1 (GLP-1). 1
- How they work for blood sugar: They help your pancreas release insulin only when blood sugar is high and block a hormone that raises blood sugar. This “glucose-dependent” system lowers the risk of dangerous lows (hypoglycemia). 2, 10
- How they work for weight loss: They slow down how fast your stomach empties (gastric emptying) and send signals to your brain that you are full, reducing appetite and quieting “food noise.” 3, 4, 5
- Why they last longer than natural GLP-1: The body’s natural GLP-1 is broken down in minutes by an enzyme called DPP-4 enzyme. These medications are designed to resist this breakdown, allowing them to work for hours or even an entire week. 2
- Beyond the basics: These drugs are pleiotropic, having multiple effects. Many offer significant protective benefits for the heart and kidneys, reducing the risk of major cardiovascular events like heart attack and stroke. 11, 12
What This Medical Review Covers
- How GLP-1 signaling affects the pancreas, stomach, and brain
- Why the glucose-dependent insulin response matters for safety
- Why these medications last longer than natural GLP-1
- How the mechanism connects to appetite, fullness, and weight loss
How GLP-1 Medications Work by Mimicking a Natural Hormone
GLP-1 medications, known as GLP-1 receptor agonists, are designed to imitate the function of a natural incretin hormone made in your intestines. After a meal, your gut releases GLP-1, which signals your body to begin the process of absorbing and managing the nutrients you just consumed. This hormone is a key player in managing both blood sugar and appetite. 1, 2
However, the body’s own GLP-1 has a very short half-life, lasting only one to two minutes in circulation. This is due to an enzyme called dipeptidyl peptidase-4, or the DPP-4 enzyme, which rapidly degrades natural GLP-1, making it too fleeting to provide a lasting therapeutic benefit for blood sugar control or weight management. 2
That longer duration matters clinically because it turns a brief after-meal signal into a therapy that can keep working between meals and, for some formulations, across the full dosing interval. In practical terms, the medication is designed to extend a normal physiologic pathway rather than replace it with an unrelated mechanism. 1, 2
The Problem: The body’s own GLP-1 is rapidly inactivated by the DPP-4 enzyme, rendering it ineffective for long-term therapeutic use. 2
The Solution: GLP-1 receptor agonists are engineered differently. Their molecular structure is modified to resist breakdown by the DPP-4 enzyme. This resistance is the key to their success, extending their half-life from a couple of minutes to many hours or even a full week, depending on the specific medication. This sustained action allows the medication to provide a steady, consistent signal to the body, unlike the rapid spike and fall of natural GLP-1. 1

Start Quiz
Find your best GLP-1 match
What kind of compare path do you want to start with?
Ready to compare options?
Compare GLP-1 providers
Coach Claire says:
Have you ever wondered about the science behind the new class of medications helping people manage type 2 diabetes and lose weight? The key is a powerful natural process that starts in your gut every time you eat. These drugs, known as GLP-1 receptor agonists, tap into that system.
Understanding how GLP-1 works is about understanding how your body is designed to regulate hunger and blood sugar. These medications don’t introduce a foreign process; they amplify a natural signal your body already uses, making it more powerful and longer-lasting to achieve a therapeutic effect. Let’s explore the science. 1, 2
A Coordinated Effort: How GLP-1s Affect the Pancreas, Stomach, and Brain
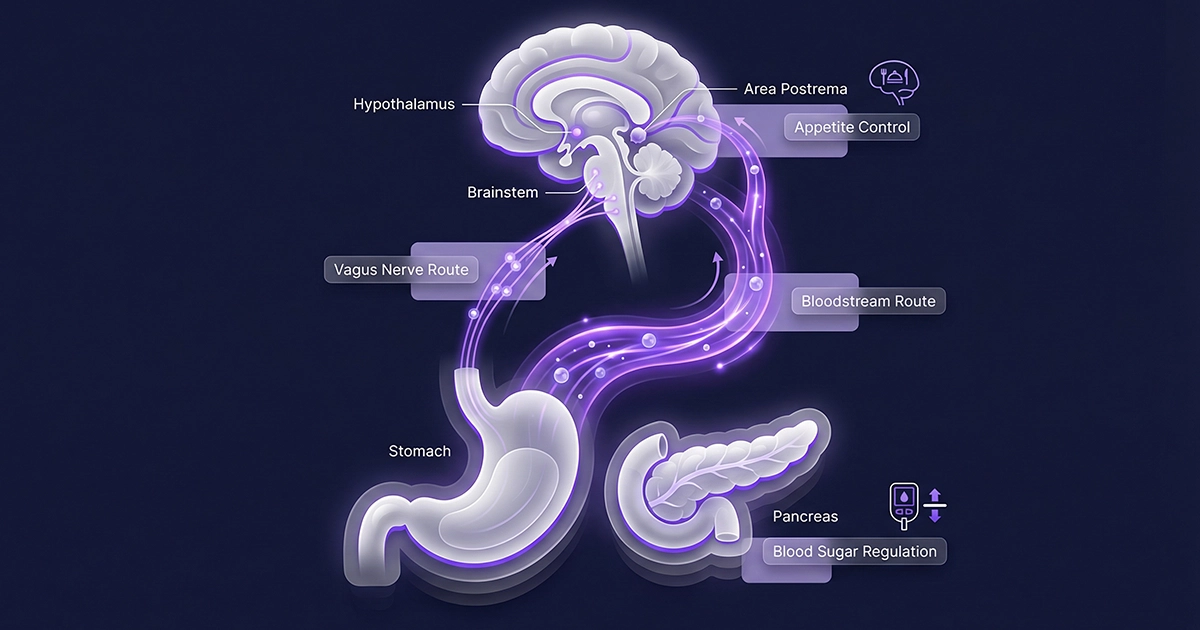
To achieve their results, GLP-1s don’t just work in one place; they orchestrate a response across several key systems in your body. This multi-organ effect is what makes them so effective. The primary targets are the pancreas, the stomach, and the brain, which communicate through a complex network known as the gut-brain axis. 3
GLP-1 signaling reaches the brain through both direct hormone signaling and broader gut-brain communication pathways involved in appetite regulation. Together, these pathways help the brain register fullness and reduce hunger. Research showing that blocking GLP-1 receptors can blunt satiety after eating underscores how important this signaling is. 3, 6
This coordinated action is central to its dual benefits for both metabolic health and weight management. 1
| Organ | GLP-1 Action | The Result |
|---|---|---|
| Pancreas | Stimulates insulin release in response to high blood sugar and suppresses glucagon secretion. | Lowers blood glucose levels after meals without causing a significant drop when sugar is already normal. 2 |
| Stomach | Slows down gastric emptying, the rate at which food leaves the stomach and enters the small intestine. | You feel full sooner and stay full for longer, leading to a natural reduction in calorie intake. 6 |
| Brain | Binds to receptors in the hypothalamus and brainstem, signaling satiety (fullness) and reducing the reward signals associated with palatable foods. | Decreases appetite, reduces food cravings, and quiets “food noise,” making it easier to manage eating habits. 4, 6, 9 |
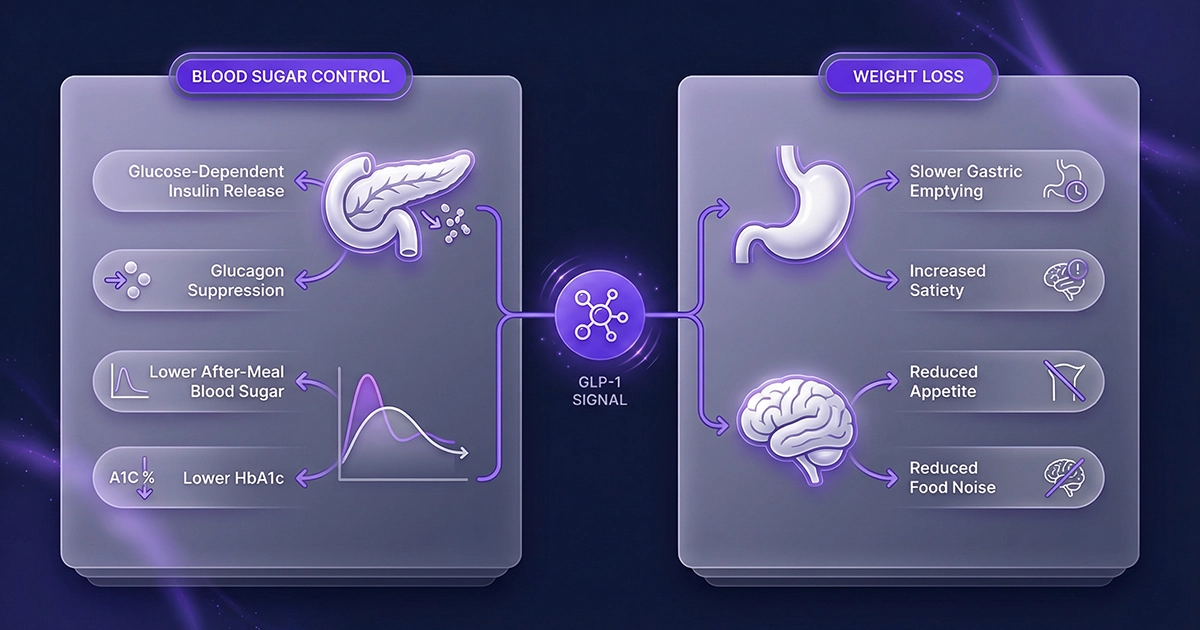
The Two-Fold Impact on Blood Sugar and Body Weight
The science of how GLP-1 works translates directly into two of the most well-known outcomes: improved blood sugar control and significant weight loss. These benefits arise from the coordinated actions in the pancreas, stomach, and brain.
For blood sugar, the mechanism is particularly intelligent. GLP-1 agonists prompt the pancreas to release insulin in a “glucose-dependent” manner. This means they primarily act when blood sugar levels are rising, such as after a meal. At the same time, they suppress glucagon, a hormone that tells the liver to release stored sugar. This dual action effectively lowers high blood sugar spikes. This improved control is reflected in lower HbA1c levels – a key long-term measure of blood sugar management – with studies showing reductions of 1% to 2% on average. 1, 10
That glucose-dependent design also helps explain why clinicians often view GLP-1 therapy differently from older drugs that drive insulin release more broadly. It supports blood sugar control while keeping the effect tied to elevated glucose, which is one reason these medicines are now used across both diabetes and obesity care. 2, 14
For weight loss, the impact comes from both the stomach and the brain. By slowing gastric emptying, GLP-1 agonists keep food in the stomach for a longer period. This physical effect contributes to a feeling of fullness. 7
Coach Claire Tip:
It’s smart to ask about safety. A key feature of how GLP-1 works is that it’s ‘glucose-dependent.’ This means it primarily boosts insulin only when your blood sugar is high after a meal. This intelligent action is why the risk of hypoglycemia (dangerously low blood sugar) is much lower compared to some older diabetes drugs like sulfonylureas. Always discuss your personal risk with your doctor, but know this safety feature is a core part of the drug’s design. 10, 14
Beyond Weight and Sugar: The Protective Effects on the Heart and Kidneys
The benefits of GLP-1 therapy are now known to extend well beyond the original targets of blood sugar and weight. These medications have pleiotropic effects, meaning they act on multiple systems in the body, including providing significant protection for the cardiovascular and renal systems. 1
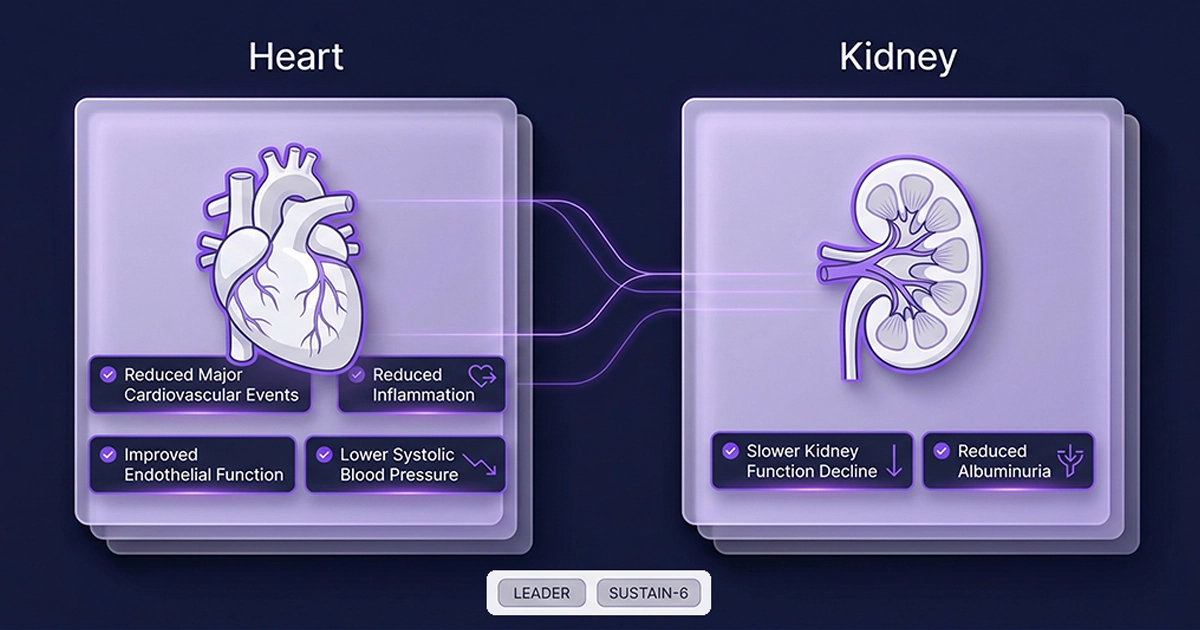
Major clinical trials have demonstrated that certain GLP-1 receptor agonists can significantly reduce the risk of major adverse cardiovascular events (MACE), such as heart attack, stroke, and cardiovascular death. For example, the LEADER trial showed this benefit for liraglutide, and the SUSTAIN-6 trial demonstrated similar outcomes for semaglutide in people with type 2 diabetes and high cardiovascular risk. 11, 12
The mechanisms behind these powerful effects are multifactorial, including indirect benefits from weight loss and improved glucose control, as well as more direct actions. Key mechanisms for cardioprotection are thought to include:
- Reduced Inflammation: GLP-1s appear to have systemic anti-inflammatory effects on blood vessels, which can slow the progression of atherosclerosis (the buildup of plaque in arteries). 1
- Improved Endothelial Function: They can help improve the health and function of the lining of blood vessels. 1
- Improved Blood Pressure: Small but clinically meaningful reductions in systolic blood pressure are consistently observed with treatment. 7
- Renal (Kidney) Protection: These drugs have been shown to slow the decline of kidney function and reduce albuminuria (an early sign of kidney damage). The risk of new or worsening nephropathy was significantly lower in people taking semaglutide in the SUSTAIN-6 trial. 8
These added benefits have made GLP-1 receptor agonists a critical therapeutic option for individuals with type 2 diabetes who are at high risk for cardiovascular and kidney disease. 9
A Comparative Look: GLP-1s vs. Other Antidiabetics
Before the advent of GLP-1 agonists, the landscape of diabetes treatment was dominated by other classes of medications, such as metformin and sulfonylureas. Understanding how GLP-1s differ highlights their unique advantages. 9
That comparison matters because these classes can improve blood sugar through different pathways and come with different tradeoffs around weight, appetite, and tolerability. 12, 13, 14
| Feature | GLP-1 Receptor Agonists | Metformin | Sulfonylureas |
|---|---|---|---|
| Primary Mechanism | Mimics incretin hormones; glucose-dependent insulin release, slows digestion, signals brain satiety. 1 | Non-GLP-1 glucose-lowering therapy. 12 | Older insulin-stimulating therapy. 13 |
| Effect on Weight | Significant weight loss. 5, 6 | Weight neutral or modest weight loss. 10 | Weight gain is common. 11 |
| Risk of Hypoglycemia | Very low when used alone. 9 | Very low when used alone. 9 | Moderate to high risk. 11 |
| Cardiovascular Benefits | Proven to reduce risk of MACE in certain drugs. 9, 10 | Not a defining cardiovascular-outcomes advantage in this comparison. 12 | Not a defining cardiovascular-outcomes advantage in this comparison. 13 |
Common Side Effects: Your Body’s Adjustment Period
While GLP-1 receptor agonists offer significant benefits, they also come with a well-known set of potential side effects, especially when starting the medication or increasing the dose. Most of these are related to the drug’s mechanism of action in the digestive system. 12
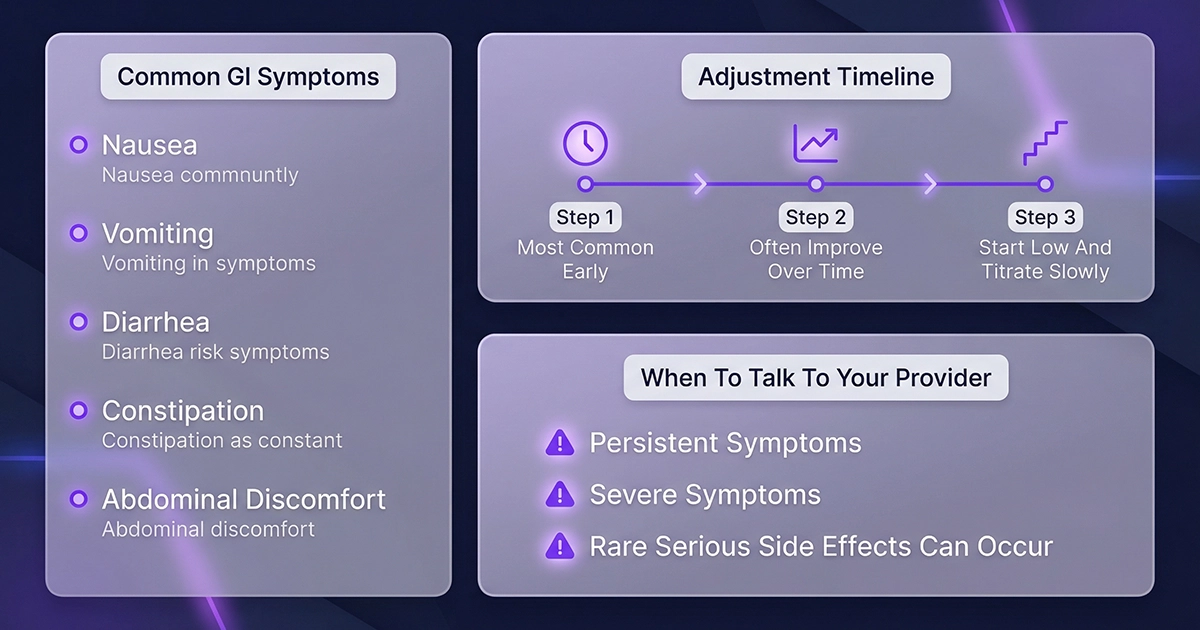
The Warning: The most common side effects are gastrointestinal. Because these drugs slow down gastric emptying, you may experience nausea, vomiting, diarrhea, constipation, or abdominal discomfort. These effects are a direct result of food staying in your stomach longer. 12
The Timeline: For most people, these side effects are most pronounced during the first few weeks or months of treatment. The body typically adapts over time, and the symptoms often lessen or resolve completely. Starting at a low dose and titrating up slowly is a key strategy used to improve tolerability. 12
Many prescribing plans intentionally begin with a lower dose and step upward over time so the digestive system has a chance to adjust. people are usually counseled to contact their clinician if nausea, vomiting, or reduced intake becomes persistent, severe, or hard to manage, especially during titration. 14
Important Safety Information:
Side effects are common but usually temporary as your body adjusts. However, you should always discuss any persistent or severe symptoms with your healthcare provider. They can help you manage side effects and ensure the medication is right for you. In rare cases, more serious side effects can occur. 12
Coach Claire’s Takeaway
Understanding the science behind GLP-1s is the first step. These medications are a powerful tool, but they work best as part of a team effort. Partner with your healthcare provider to build a complete plan that includes nutrition, movement, and the right medical support for you. You’ve got this.
Frequently Asked Questions
How quickly do GLP-1 medications start to work?
You may notice effects on your appetite within the first few weeks, but the full effects on blood sugar (as measured by HbA1c) and weight loss can take several months to become apparent. The impact builds as the dose is gradually increased to the target maintenance level according to the prescribing information. 12
Is GLP-1 a type of insulin?
No, GLP-1 is not insulin. It is a hormone-mimicking drug that helps your own body release insulin more effectively in response to glucose. It does not replace the need for insulin in individuals with type 1 diabetes. 1
Can I stop taking a GLP-1 agonist once I lose weight?
GLP-1 receptor agonists are considered long-term treatments for chronic conditions like type 2 diabetes and obesity. Their effects on appetite and blood sugar are present only while you are taking the medication. Stopping the medication often leads to the return of appetite and potential weight regain. Always consult your doctor before making any changes to your medication regimen. 12
Why are most of these drugs given as injections?
GLP-1 agonists are biologic drugs (peptides). If taken orally as a standard pill, they would be broken down by stomach acid and digestive enzymes, just like the protein in food. Injections allow the medication to be absorbed directly into the bloodstream without being destroyed. An oral formulation of semaglutide is available, which uses special technology to protect the medication from stomach acid. 13
Coach Claire’s Cheat Sheet
Quick definitions used in this article.
Medical disclaimer: This content is for educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed healthcare professional before starting, stopping, or changing any medication or care plan.
References
- Drucker, D. J. (2018). Mechanisms of Action and Therapeutic Application of Glucagon-Like Peptide-1. Cell Metabolism. https://pubmed.ncbi.nlm.nih.gov/29617641/ [top]
- Nauck, M. A., & Meier, J. J. (2018). Incretin hormones: Their role in health and disease. Diabetes, Obesity and Metabolism. https://pubmed.ncbi.nlm.nih.gov/29364588/ [top]
- Liu, Q. K. (2024). Mechanisms of action and therapeutic applications of GLP-1 and dual GIP/GLP-1 receptor agonists. Frontiers in Endocrinology. https://pubmed.ncbi.nlm.nih.gov/39114288/ [top]
- Cabou, C., & Burcelin, R. (2011). GLP-1, the gut-brain, and brain-periphery axes. Reviews in Diabetic Studies. https://pubmed.ncbi.nlm.nih.gov/22262078/ [top]
- Krieger, J. P., Langhans, W., & Lee, S. J. (2015). Vagal mediation of GLP-1’s effects on food intake and glycemia. Physiology & Behavior. https://pubmed.ncbi.nlm.nih.gov/26048300/ [top]
- Melhorn, S. J., et al. (2014). Initial evidence that GLP-1 receptor blockade fails to suppress postprandial satiety or promote food intake in humans. Appetite. https://pubmed.ncbi.nlm.nih.gov/25049134/ [top]
- Aldawsari, M., et al. (2023). The Efficacy of GLP-1 Analogues on Appetite Parameters, Gastric Emptying, Food Preference and Taste Among Adults with Obesity: Systematic Review of Randomized Controlled Trials. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy. https://pubmed.ncbi.nlm.nih.gov/36890965/ [top]
- Farr, O. M., et al. (2016). GLP-1 receptors exist in the parietal cortex, hypothalamus and medulla of human brains and the GLP-1 analogue liraglutide alters brain activity related to highly desirable food cues in individuals with diabetes: a crossover, randomised, placebo-controlled trial. Diabetologia. https://pubmed.ncbi.nlm.nih.gov/26831302/ [top]
- Marso, S. P., et al. (2016). Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. New England Journal of Medicine. https://www.nejm.org/doi/full/10.1056/NEJMoa1603827 [top]
- Marso, S. P., et al. (2016). Semaglutide and Cardiovascular Outcomes in people with Type 2 Diabetes. New England Journal of Medicine. https://www.nejm.org/doi/full/10.1056/NEJMoa1607141 [top]
- American Diabetes Association. (2024). 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes – 2024. Diabetes Care. https://diabetesjournals.org/care/article/47/Supplement_1/S158/154089/9-Pharmacologic-Approaches-to-Glycemic-Treatment [top]
- Foretz, M., et al. (2019). The mechanisms of action of metformin. Diabetologia. https://pubmed.ncbi.nlm.nih.gov/28776086/ [top]
- Costello, R. A., Nicolas, S., & Shivkumar, A. (2026). Sulfonylureas. StatPearls [Internet]. https://pubmed.ncbi.nlm.nih.gov/30020597/ [top]
- U.S. Food & Drug Administration (FDA). (2025). WEGOVY (semaglutide) injection, for subcutaneous use, prescribing information. fda.gov. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/215256s024lbl.pdf [top]
- U.S. Food & Drug Administration (FDA). (2025). RYBELSUS (semaglutide) tablets, for oral use, prescribing information. fda.gov. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/213051s024,s028s029lbl.pdf [top]